
Breast Reconstruction
Performed by Dr. Bosshardt
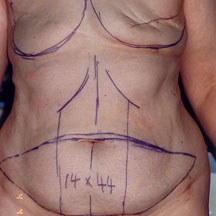

Before
After

61 year old patient underwent a right modified radical mastectomy in 1976 and a left mastectomy in 1996 for breast cancer. After the second procedure, the patient sought reconstruction. She is seen marked for surgery. The large, spindle-shaped area of skin and fat on the lower abdomen, marked �14 x 44 (cm)� will be divided in half and each half used to build one breast.
Patient is shown one year and nine months after reconstruction of both breasts with TRAM (using abdominal muscle, skin, and fat) flaps and nipple/areola reconstruction with nipple flaps and medical tattooing. Bra cup size is a D.


Before Side View
After Side View
This 47 year old patient had a left modified radical mastectomy for breast cancer and underwent reconstruction with an implant elsewhere. She had postoperative radiation therapy and this caused the tissue around her implant to scar and contract, producing a small, hard breast mound which felt and looked nothing like her natural breast. Radiation therapy can be very damaging to normal tissues and usually implant reconstruction does not work well in such patients.
Here she is 1 year and 9 months after removal of her breast implant and a new breast reconstruction using skin and fat from her abdomen (this is called a TRAM flap for Transverse Rectus Abdominis Myocutaneous flap) followed by reconstruction of the nipple area with a small flap and tattooing of the color. This flap allows the surgeon to remove a lot of the radiation damaged tissue and replace it with healthy, pliable abdominal tissue. This new breast, though not perfect, is just as soft and natural as her right breast and should remain so forever.


Before
After
Poland�s Syndrome Reconstruction
This patient has a severe expression of Poland�s Syndrome, in which the breast and underlying pectoralis major muscle are absent. She had undergone two previous attempts at reconstruction elsewhere, without success, due to infection. She is shown before and after reconstruction. The right breast was lifted and the left breast reconstructed using a tissue expander, followed by insertion of a permanent implant. The nipple/areola complex was reconstructed using skin from the right areola and a small flap to simulate the nipple. The implant is a Mentor adjustable saline implant with a volume of 730 cc. She wears a D cup bra and fills both cups very evenly. This patient takes a long time to settle her scars, which remain very red for a long time.


This young woman had cancer of the right breast. She underwent a right mastectomy and reconstruction with immediate placement of a tissue expander. This was later replaced with a permanent implant and she underwent nipple/areola reconstruction using a nipple sharing technique with medical tattooing of the areola. Since the left nipple was generous, reducing it improved the left breast and provided nipple tissue for the right (the Robin Hood principle of plastic surgery). She also had breast augmentation on the left. Her implants are McGhan textured, anatomically-shaped, saline implants; 390 cc on the right and 230 cc on the left. She is shown just after her breast biopsy and after the completed reconstruction.


Before
After
(Before) - This case spans nearly 13 years, going back to 1992 when this 35 year old patient was first diagnosed with cancer of the left breast. She is shown before her mastectomy, marked for removal of the nipple/areola and biopsy site. Reconstruction was planned using a flap of skin and muscle from the back (latissimus dorsi muscle) with a small, textured saline implant.
(After) - Patient underwent a planned preventative mastectomy on the right with immediate reconstruction using an abdominal flap (TRAM flap). Cancer was found in this breast and she underwent an immediate mastectomy, without reconstruction. After a course of chemotherapy and radiation, she came back to finish the reconstruction on the right. This photograph shows her after the completed reconstruction. The left breast has held up beautifully with only the one implant exchange for a leaking implant, and a single repigmentation of the areola. So far, she continues to be free of cancer.


Before
After
(Before) - This 41 year old patient presented with an extremely difficult situation for breast reconstruction. She had a left mastectomy for breast cancer and a right mastectomy for prevention of future cancer because of her cancer type. She also had radiation therapy to the left side (note the darkened skin). Her slim figure made it impossible to build two breasts with her own tissue. The left breast was reconstructed with an abdominal (TRAM) flap with later tissue expansion and an implant, and her right with tissue expansion and an implant. I first saw her in July 2002. She underwent a total of 5 procedures; 3 to build the two breasts mounds, and 2 to reconstruct the nipples and areolae.
(After) - She is shown in May 2005. While symmetry is not perfect, she has a good match, the breasts are soft, and she can wear any clothes she wishes without a prosthesis.