(The top photo her implants are 500 cc. In the bottom photo her implants have been switched out to a pair of 600 cc )


Imagine the possibilities.
(The top photo her implants are 500 cc. In the bottom photo her implants have been switched out to a pair of 600 cc )
.jpg)
Well, it was thirty five years in the making and over twenty years in the writing, re-writing, and endless editing. What started as one book became two. The first takes you on a two year roller coaster ride of emotions and new experiences as I learn the scope and breadth of my chosen profession and struggle to assimilate the mass of information and acquire the skills necessary to practice independently and, more important, competently and safely. It was the hardest two years of my life, coming after a full five years of training to become a general surgeon. There were times when I thought I would never make it.
Most people do not really know what a plastic surgeon is, what it takes to become a fully-trained, board-certified plastic surgeon. I understand because even after I decided to dedicate my professional life to this, I really had no clue myself. Plastic surgeons are not merely "nip and tuck" surgeons performing cosmetic surgery on an endless procession of vain, well-to-do patients. They manage trauma, some of it horrendous, like the little boy run over by a boat propeller. They treat jaw fractures and other facial fractures. They repair congenital deformities like cleft lips and palates. They reconstruct breasts lost to cancer. They treat the horrific deformities from severe burns. They do hand surgery, including replantation of amputated limbs. They reconstruct faces after accidents and removal of sometimes huge skin cancers. They are the only surgeons who truly work from the top of the head to the toes, assisting other surgeons with their unique skills.
Although plastic surgery continues to be destigmatized and resources for breast cancer treatment and prevention continue to grow, the number of women who were offered reconstructive surgery after a mastectomy does not reflect that. ??
As of 2017, less than half of all women who required a mastectomy were offered breast reconstruction surgery, and fewer than 20% opted for immediate reconstruction. ?
What many patients don’t know is having a plastic surgeon on your breast cancer team can make a huge difference. ?#BreastReconAwareness
Special Shoutout and Congrats to Dr Bosshardt for 30 years of membership in the America Society of Plastic Surgeons. Woohoo!

Mold, fungi, yeast. They are literally everywhere. Yeast are so ubiquitous that you can make sourdough bread starter just by leaving some warm water mixed with flour out in the open for a few days. Yeast from the environment will populate the liquid and ferment the flour. Likewise, mold and fungi are found anywhere there is a dark, mildly humid environment. This has not changed from time immemorial.

We are all tired of being home and are ready to hit the beach this summer. So start getting that beach bod ready now with this special summer "Mommy Makeover Summer Special"!
We are offering two awesome services to get you swimsuit ready, Breast Augmentations and Tummy Tucks. During this special limited-time offer, combine them both and you can save even more money!
It's all anyone can talk about these days.  Covid-19 has taken over every aspect of our lives, and the hot debates continue over how to proceed to protect the citizen and the hard hit economy.
Covid-19 has taken over every aspect of our lives, and the hot debates continue over how to proceed to protect the citizen and the hard hit economy.
Click HERE to read Dr. Bosshardt's blogs on his thoughts of the virus.


A slim 32 year old woman came to see me for breast implants. The year was 1998. The breast implant crisis, courtesy of Connie Chung's expose, was still going strong. Silicone gel implants were off the market for all but reconstruction and only saline implants could be used for augmentation. While the demand for implants plummeted, there was still no lack of young women seeking these.

To schedule your complimentary breast augmentation consultation, call Amy at 352-742-0079.
“Mohs, which stresses taking thin margins, has no place in treating invasive melanoma.”
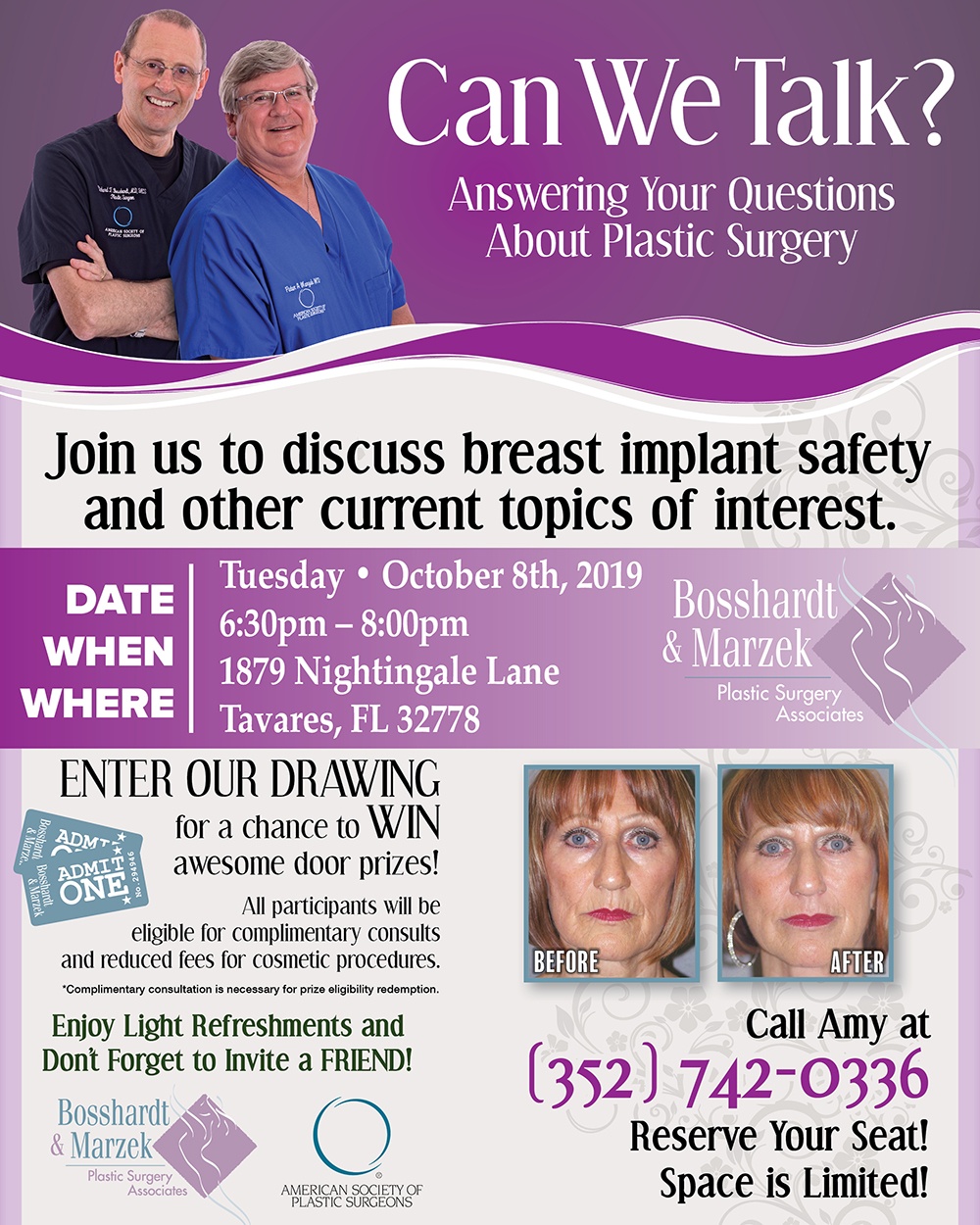
Join us to discuss breast implant safety and other current topics of interest. This is a FREE EVENT, however, seating is limited so please RSVP to Amy at 352-742-0336.

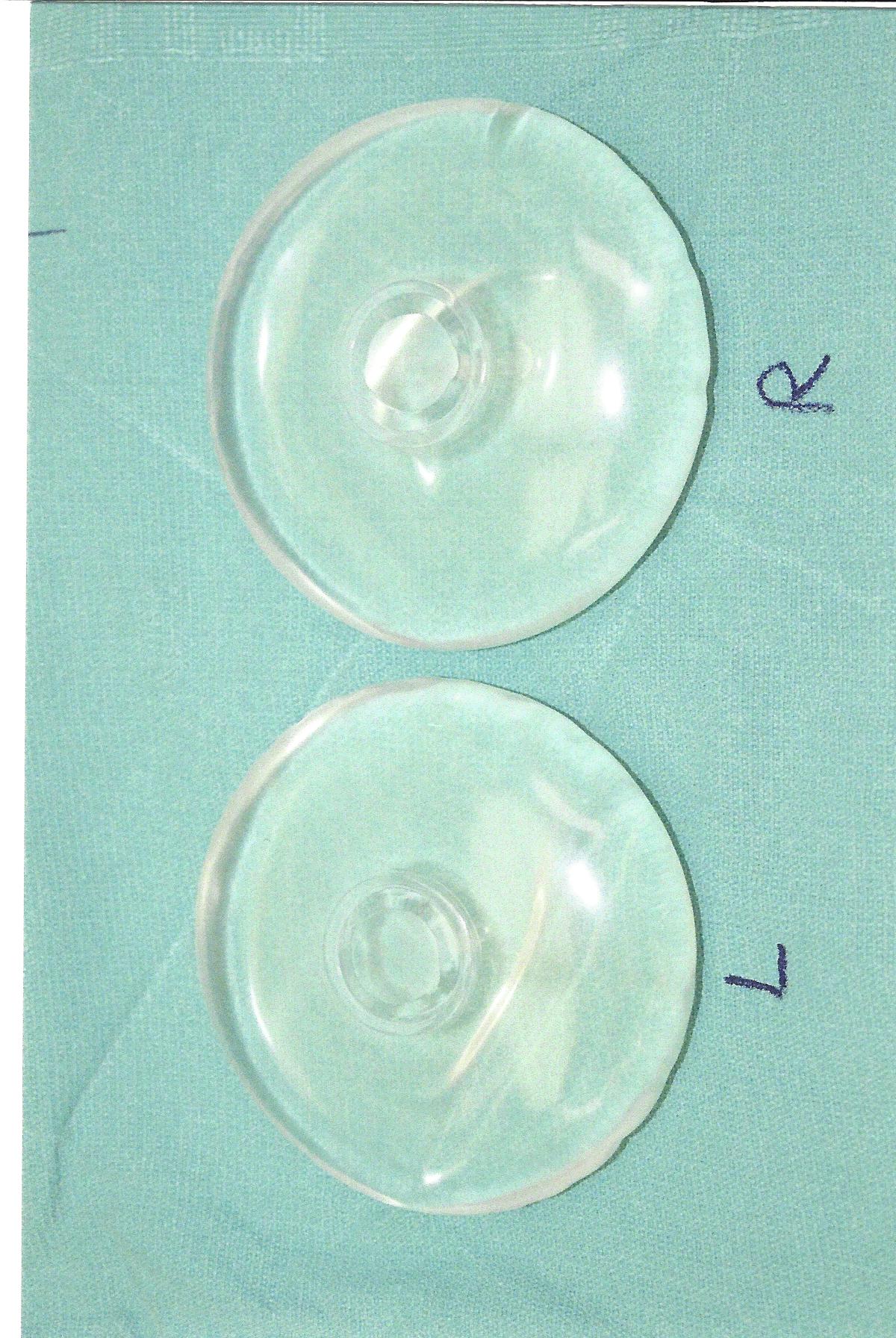
This 78 year old woman came to see me because of swelling of her right breast. She had breast augmentation performed in 1984 with what she believed to be saline implants. She had no paperwork on them. Although her breasts became firm over the years, she had no other problems with them and was happy with the result. Her overall health was excellent with only some hypertension that was treated. She had a mammogram in 2018 that was reported to her as OK.

For nearly the entire thirty years that I have been in practice, some women have claimed that breast implants made them sick. This controversy came to a head around 1991 when the first implant crisis exploded in the wake of Connie Chung’s expose on television. After a more than a decade of media hysteria, thousands of law suits, and a flurry of reports from major medical centers, it seemed that implants were exonerated, unlike President Trump, and the issue essentially disappeared. It was not totally gone, however, just smoldering, waiting to rise, like a Phoenix from the ashes, with the next wave of accusations.
The next wave is now here, abetted by the game changer and force multiplier, social media. There have always been women who suspected their implants were making them sick but many, if not most, have been marginalized by physicians and plastic surgeons who did not take their complaints seriously. Until social media, most felt as though they were in this alone. Now, websites allow women with concerns to share their stories with others who have experienced similar problems, obtain affirmation for their condition, and strength in numbers.

Social media and the mainstream media are full of posts and articles, respectively, regarding the issue of breast implant associated lymphoma, the ban in several countries of use of Allergan’s textured biocell implants, and, most recently, of Allergan’s voluntary removal from the U.S. market as well. Here are some facts about the situation.

We have “young gun” newly elected politicians with little knowledge of history or the political process itself pushing legislation and policies that are either patently unrealistic, absurd, or simply modern sounding versions of tired, failed ideas of the past. The poster child for this seems to be Alexandra Ocasio Cortez who utters idiotic ideas with a level of confidence that I can only envy. What is truly frightening is that she now has a platform from which to spout her inanities and a small but real audience of equally clueless followers.

“Doctor, will I have a scar?” This question comes up in many, if not most, discussions related to an injury or surgery. Underlying the question is concern regarding appearances and possible disfigurement following one or the other.
In 30 years of practice as a plastic surgeon, I have not had even half a dozen patients return to me with the type of non-specific, multi-system complaints often attributed to what is being called “breast implant illness” or BII. Is BII real? I don’t know and neither, it appears, does anyone else. Are there women out there with poorly understood, unexplained disorders who have breast implants? Of course. There are also millions of women with these same disorders who have never been in the same room with a breast implant. Among the many things you learn after a few years of practice is that, in the world of medicine, anyone can react badly to anything. It can be a drug, metal, latex, gluten, or any other of the countless things we are exposed to in some manner and, yes, I would include breast implants. Why should implants be any different? It is another thing to claim, however, as some are doing, that implants are inherently dangerous, toxic devices that will make everyone who has them sick eventually. This flies in the face of reason and decades of experience with implants.
I had a very interesting patient return to me recently. Bea (not her real name) came to me in 2008 seeking breast enhancement. Her breasts were sadly deflated and sagging after having children. The areolae were stretched out. I suggested a breast lift followed by placing implants at a second procedure and she went ahead. Her result was great and both of us were very pleased. Over the subsequent years, I saw her for a couple of minor procedures, with the last aournd 5 years ago. She remained completely pleased with her breasts.

I love getting 5 star reviews on Google and similarly stratospheric reviews on vitals.com, realself.com, and healthgrades.com. What’s not to like? A lot, actually. You see, if you look carefully, interspersed in those 4 and 5 star reviews are several 1 star reviews. A 1 star review means you are one step above, say, a child abuser or serial killer. In other words, you are so bad that the reviewer went as low as the process would allow. I know this is so because in the comments are such pearls as “Horrible “Dr.””, “…..You disgust not only me but my husband says the same….Run, run” (not sure if she means me or my patients should run).

The decision to have a breast augmentation is a major one with life-long consequences. Please be sure you understand this operation well and have all of your questions answered before proceeding. Once surgery is done, it can never be totally undone.
The email began, “Congratulations are in order. Your practice has been selected to be featured in Americastopbreastsurgeons.com.” Wow! Really? At last, my incredible talents have been properly recognized. With fingers trembling in gratitude, I click to go to the site and claim my recognition. But wait…….what’s this? Even though it claims to be some type of award or distinction, I have to pay for a membership. Membership? Since when do you have to pay for receiving an honor? Membership is what you do when you join a club. “Membership” among America’s Top Breast Surgeons is $500 for one year, $1000 for life, and $2000 for “#1 Top Spot membership. If I want my practice listed, it is $995 for 6 months, $1895 for one year, $2895 for lifetime membership, and a mind-boggling $3895 for the #1 Top Spot. My mind reels with questions. Is this for real? How did I come to the attention of those who select ATBS’s? Who nominated me? How many doctors in my area received similar emails? Did my partner receive an invitation? Do I act quickly if I want #1 Top Spot ranking?
Is there such a thing as ‘Breast Implant Illness”, a unique condition found in women with breast implants? With over 5 million women with implants in the U.S.A. alone, this would seem to be an important question to answer. Are there women who have breast implants and experience a dizzing array of medical symptoms? Of course. As of 2010, over five million women in the U.S. have had breast implants inserted. In any group so large, you are going to have women with all sorts of complaints or disorders. The question then becomes, are these caused by their implants, all or in part, or not?

I recently saw an 80 year old man. Ten years ago, he had a squamous cell skin cancer on his scalp. His dermatologist recommended radiation therapy. Eight years later, the treated area broke down spontaneously and for two years he has had an ulcer on top of his head that has resisted all efforts to get it healed. On his examination now, he has a 2. 5 cm (1 inch) round ulcer on top of his head. The base of this ulcer is bare bone. The surrounding scalp is fibrous with no elasticity and clearly poor blood circulation. Getting this ulcer healed will require major surgery, if it can be done at all.

Ironically, It is the holy grail of plastic surgery. I say ironic because it is not really surgery at all. What is it? It is the removal of unwanted fat and tightening loose skin without having to go through an operation with its attendant costs, risks, postoperative pain, and scars. Surgery, of course, can remove large quantities of fat and tighten skin as nothing else can but has all of the aforementioned issues, making it an unattractive option for many people.
 Patients often ask me what they can do to prepare themselves for an upcoming surgical procedure. I love this. It means the patient is invested in the surgery and actively working with me to get the best result.
Patients often ask me what they can do to prepare themselves for an upcoming surgical procedure. I love this. It means the patient is invested in the surgery and actively working with me to get the best result.
I believe the single most significant factor under a patients control is to avoid tobacco in all its forms. Smoking is, I feel, the single biggest lifestyle factor that can adversely affect surgery. In addition to being one of the worst habits anyone can engage in- I semi-seriously tell patients they would be better off shooting heroin than smoking- smoking puts patients at greater risk of surgical complications. Nicotine containing products, such as patches or gum should also be stopped. Nicotine is a potent vasoconstrictor; it causes blood vessels to clamp down for up to 24 hours. This reduces blood flow to areas, especially skin, and, combined with surgical manipulation, can reduce blood flow below a critical level where skin and other soft tissues will die. Smoking's ill effects are so serious that I will not perform certain elective operations unless the patient stops for a minimum of four weeks before surgery and does not resume for three to four weeks afterward. These include facelifts, breast lifts and reductions, tummy tucks, and any operation where the skin will be lifted and tightened. The risks just aren't worth it.
Patients often ask about drinking alcohol before surgery. I have no problem with patients having a glass of wine, beer, or a single mixed drink on the evening before surgery. I don't feel this has any clinically significant effect on bleeding. I don't want patients inebriated the night before surgery or drinking heavily in the weeks leading up to surgery. Excessive alcohol intake creates enough problems of its own without adding this to the lead to surgery. Alcohol, like other sedatives, can affect a patient’s ability to metabolize and respond appropriately to many drugs used for anesthesia. Alcohol in excess damages the liver and this organ is crucial to the metabolism of a large spectrum of drugs as well as producing factors necessary for blood clotting.

Young women seeking breast implants often ignore a critical aspect of this surgery: they will have these implants in their breasts for years, even decades. What happens to them over time? This is an aspect of breast implant surgery that I feel many surgeons gloss over. What are the long term consequences of having breast implants?
 If you are diagnosed with skin cancer, your doctor may recommend surgery to remove the cancer and prevent it from spreading. Depending on the type of skin cancer you are diagnosed with and the amount of skin and tissue around the cancer that must be removed, your Oncologist may recommend that you have reconstructive surgery to replace skin and tissue and minimize scarring.
If you are diagnosed with skin cancer, your doctor may recommend surgery to remove the cancer and prevent it from spreading. Depending on the type of skin cancer you are diagnosed with and the amount of skin and tissue around the cancer that must be removed, your Oncologist may recommend that you have reconstructive surgery to replace skin and tissue and minimize scarring.
Our plastic surgeons are highly trained in the reconstruction necessary following skin cancer removal. They possess extensive knowledge in the latest and most effective surgical techniques. Our plastic surgeons have performed a wide range of skin grafts and tissue transfer procedures.
They are fully skilled at the superior restoration of the skin cancer site so that it matches the remaining skin. Because they closely work with other experts in the field, they can call on any other type of medical expert needed right at our facility, including pathologists, oncologists, and dermatologists.
It may surprise many people that many plastic surgeons perform a lot of hand surgery. Both orthopedic and plastic surgeons receive extensive training in hand surgery during their residency programs, and hand surgery is an integral part of plastic surgery. Some surgeons go on to do additional training to specialize in hand surgery.
 You may be referred to plastic surgery for a broad range of hand problems. We do lots of trauma care involving hand injuries. These include such things as tendon repair, repair of hand fractures, and repair of complex soft tissue injuries of the hands and fingers. In the area of elective surgery, you may be sent to a plastic surgeon for removal of tumors or skin cancers of the hands; for problems related to Dupuytren's contracture, an unusual condition in which fibrous bands in the palms gradually cause the fingers to bend and remain bent; for carpal tunnel surgery to relieve pressure on nerves in the wrist than can affect hand function and sensation, for trigger fingers; and for ganglions of the fingers and wrist.
You may be referred to plastic surgery for a broad range of hand problems. We do lots of trauma care involving hand injuries. These include such things as tendon repair, repair of hand fractures, and repair of complex soft tissue injuries of the hands and fingers. In the area of elective surgery, you may be sent to a plastic surgeon for removal of tumors or skin cancers of the hands; for problems related to Dupuytren's contracture, an unusual condition in which fibrous bands in the palms gradually cause the fingers to bend and remain bent; for carpal tunnel surgery to relieve pressure on nerves in the wrist than can affect hand function and sensation, for trigger fingers; and for ganglions of the fingers and wrist.
Some plastic surgeons that specialize in hand surgery can offer highly technical and complex care such as microsurgery, joint replacement, major hand reconstruction, tendon transfers, nerve and blood vessel repairs, and more.
 The short answer is no. The more comprehensive answer is, it depends. It depends on what type of liposuction you are discussing. There are two general categories of liposuction: large volume and small volume.
The short answer is no. The more comprehensive answer is, it depends. It depends on what type of liposuction you are discussing. There are two general categories of liposuction: large volume and small volume.
Large volume liposuction is performed in patients who are overweight or obese and seeking removal of a large amount of fat. Most plastic surgeons agree that this would be 5 liters of fat or more at one time, about one and a quarter gallons for the non-metric types. Large volume liposuction is not a cosmetic procedure although it may produce cosmetic benefits. It is major surgery and should be done in a hospital setting with overnight monitoring because of the potential for major effects on such things as blood pressure and heart, kidney, and lung function. Deaths from liposuction have been primarily in patients undergoing large volume liposuction. In some patients who are obese and have diabetes, large volume liposuction has been shown to provide some improve in blood sugar control.
Most liposuction done today removes much less than 5 liters and is done for body contouring. In many cases, the benefit may be seen more in how your clothes fit and how you look, than what you scales show. If you are stable in your weight and have specific areas of concern, then liposuction can help you work towards your goal.
 Many patients ask what typical recovery times are after our most popular plastic surgery procedures. This depends on many things of which the type of surgery is only one. First, what is meant by “recovery time”? Is this when you will look presentable, when you will be able to resume normal day to day activity, or when you can resume all activities, with no restrictions? Is it when you can return to work? This can be very different for a secretary who works at a desk versus, say, someone who does heavy manual labor. Each of this may have a different time frame, from days to weeks. Is it when you will feel back to totally normal in every way? This could be months. Scars can take six months to over a year to fully mature. It is important always to remember that each individual will recover in their own, unique way and so we have to allow some leeway for this in our estimations.
Many patients ask what typical recovery times are after our most popular plastic surgery procedures. This depends on many things of which the type of surgery is only one. First, what is meant by “recovery time”? Is this when you will look presentable, when you will be able to resume normal day to day activity, or when you can resume all activities, with no restrictions? Is it when you can return to work? This can be very different for a secretary who works at a desk versus, say, someone who does heavy manual labor. Each of this may have a different time frame, from days to weeks. Is it when you will feel back to totally normal in every way? This could be months. Scars can take six months to over a year to fully mature. It is important always to remember that each individual will recover in their own, unique way and so we have to allow some leeway for this in our estimations.
Facial surgery is more difficult to hide than surgery in areas covered by clothes, and this must be taken into account as well.
Most patients can return to full, unrestricted activity after any surgery within 4-6 weeks. Most can look presentable, even after facial surgery (makeup can hide a myriad of things like bruising and redness) within 7-10 days. With the above factors in mind, the following is a list of average recovery times -- when you will look OK and be able to function in normal day to day activities after our most common and popular procedures:
After the blockbuster success of the movie, Jaws, in driving moviegoers out of the ocean in droves, the tagline for Jaws 2, simply said, “Just when you thought it was safe to go back into the water…..”. This could serve equally well for any number of situations in medicine. One of these is the issue of breast implant safety.
Recent media stories about the possible connection between breast implants and a rare lymphoma of the breast have made it important that women be updated on this issue.
After a decade of some of the most intense media scrutiny, claims and counter claims, and arguably the most concentrated research in the history of any medical device extending over a decade, from 1990 into the new millennium, it seemed that the question of whether or not implants could make women sick or cause cancer had been put to rest. Like a phoenix rising from the ashes, however, the issue won’t stay dead. Concerns have been raised by women’s groups and some medical professionals about possible systemic illnesses, immune disorders, and a slew of ill-defined symptom complexes blamed on implants. Scientifically proven, reproducible proof of causality has been hard to come by. Then it was discovered that there did, indeed, appear to be a true association of breast implants with a rare form of lymphoma, anaplastic large cell lymphoma, in the breast. The association is such that this has now been officially labeled breast implant associated anaplastic large cell lymphoma (BIA-ALCL) to distinguish it from ALCL not associated with implants.
 One of the most frequently asked questions about cosmetic surgery concerns scarring. The ideal is to have a successful cosmetic procedure and have no scars at all. Unfortunately, we are surgeons, not magicians, and scars are a fact of life. Many techniques have been tried to reduce or eliminate scars. Some have come and gone. Others have stayed. One of these is endoscopic surgery. It has been applied to many procedures, including breast augmentation. On the surface endoscopic breast augmentation through the armpit sounds like a winner. You get breast implants, no scar on your breasts, and only a tiny scar in the armpit. What's not to like? Well, there is more to it than that. There always is.
One of the most frequently asked questions about cosmetic surgery concerns scarring. The ideal is to have a successful cosmetic procedure and have no scars at all. Unfortunately, we are surgeons, not magicians, and scars are a fact of life. Many techniques have been tried to reduce or eliminate scars. Some have come and gone. Others have stayed. One of these is endoscopic surgery. It has been applied to many procedures, including breast augmentation. On the surface endoscopic breast augmentation through the armpit sounds like a winner. You get breast implants, no scar on your breasts, and only a tiny scar in the armpit. What's not to like? Well, there is more to it than that. There always is.
Endoscopy, surgery via small incisions using a lighted device called an endoscope, is the proverbial hammer in search of a nail. As with lasers, it has been over-hyped and some practitioners have tried to promote it for procedures where it provides no real advantage and actually creates problems. While it has revolutionized many areas of surgery, it has had limited application for plastic surgery. Much of what plastic surgeons do involves the need for larger incisions and this effectively negates one of the biggest advantages of endoscopic surgery.
Today I'm going to cover five of the biggest myths regarding breast reduction surgery.

Five benefits of a breast reduction
The transgender issue has erupted on the media and social landscape, seemingly out of nowhere. We are told by the media that this is a significant social issue that requires urgent attention, instead of the rare disorder that it really is. Legislators are already passing legislation that forces teenage girls to share their bathrooms with teenage boys who claim to be confused as to their gender. The situation has rapidly escalated to a degree that grotesque solutions are being offered, such as giving confused teens hormones to delay puberty- something that we know stunts skeletal growth and can create other medical issues- in order to facilitate gender reassignment surgery later! What is remarkable and truly worrisome is that these ridiculous "solutions" are being taken seriously. We have truly entered the realm of the absurd.
Who has not read of the strange journey and transformation of former Olympian, Bruce, now Caitlyn, Jenner? If ever there was a poster child for an issue it would be him/her. I can't speak personally regarding Jenner's situation. He may truly be a woman "trapped" in the body of a man. On the other hand, we know that gender is genetically determined. Yes, errors do occur in a very rare individual who is born with ambiguous genitalia and an abnormal set of sex chromosimes. We are not talking here about such a rare disorder. Transgendered people of the type that have suddenly become almost fashionable, are biologically normal, genetically normal males and females who simply believe that they are really the opposite sex. In medicine, we have a term for a fixed belief that runs counter to reality. We call this a delusion. We see this in anorexia nervosa and body dysmorphic disorder where people hold to a false belief, even to the point of physically harming themselves or seeking inappropriate surgical alteration. In these individuals, we do not encourage the delusion by affirming the false belief. We treat them with psychotherapy and, when appropriate, medications to normalize their thinking processes. Why do we treat transgender differently? While much is made of Jenner's transformation and wonderful life since, the truth is that long term studies clearly suggest that these unfortunate individuals often do not achieve the happiness and contentment they seek and that the incidence of suicide is up to twenty times that of their peers who do not undergo gender reassignment.
The full text of an article I wrote on the subject follows:
 While plastic surgery fashion comes and goes, some procedures remain perennial favorites. Each year the American Society of Plastic Surgeons produces its list of the most popular procedures based on a nationwide survey of plastic surgeons. Of course, there will be some variations between some parts of the country and others, but at least this lets you know what the current trend is. Changes in our demographics have led to some of the changes as well with increasing popularity of procedures dealing either with weight gain or the converse, loss of weight. Non-surgical options such as skin peels, injectable fillers, Botox, and a variety of "non-surgical" procedures and devices (some effective and some not) continue to grow in popularity as many patients want to achieve some improvements and enhancements without the cost, risk, or downtime of surgery. Sometimes, however, surgery is the only feasible, practical option.
While plastic surgery fashion comes and goes, some procedures remain perennial favorites. Each year the American Society of Plastic Surgeons produces its list of the most popular procedures based on a nationwide survey of plastic surgeons. Of course, there will be some variations between some parts of the country and others, but at least this lets you know what the current trend is. Changes in our demographics have led to some of the changes as well with increasing popularity of procedures dealing either with weight gain or the converse, loss of weight. Non-surgical options such as skin peels, injectable fillers, Botox, and a variety of "non-surgical" procedures and devices (some effective and some not) continue to grow in popularity as many patients want to achieve some improvements and enhancements without the cost, risk, or downtime of surgery. Sometimes, however, surgery is the only feasible, practical option.
In 2015, the last year for which figures are available, there were 1.7 million cosmetic operations performed in the U.S., a 115% increase over the year 2000. In 2015, the five most popular procedures were:
Young women whose breasts never developed fully and who feel disproportionately small.
The decision to have a breast augmentation is a major one with life-long consequences. Please be sure you understand this operation well and have all of your questions answered before proceeding. Once surgery is done, it can never be totally undone.
The only way to add meaningful volume or fullness to your breasts is to use breast implants. You cannot do exercises, take pills, use creams, or use “vacuum pumps” to accomplish this goal!! Some surgeons are using fat grafts to enlarge breasts. This procedure has not been widely adopted because there are still lingering questions about the long term effects of injecting one’s own fat into the breasts. The process usually requires more than one operation and rarely increases breast size more than ½ - 1 cup size. I do not feel confident enough in this procedure to offer it to my patients.
For a while, the Lifestyle Lift company founded by ear, nose, and throat doctor David Kemp was the largest purveyor of facelifts in the U.S. with over a hundred centers performing his trademarked procedure across the country. Almost overnight it was gone. It was the modern medical equivalent of the carnival folding its tents and slinking off into the night except that in this case, it has not yet popped up somewhere else. Give it time. There is too much profit in cosmetic surgery for someone not to try to resurrect it in some new incarnation.
The company failed for two reasons. It over-extended itself with its ruinous advertising budget and it sank under the weight of too many unfavorable reviews from those who were misled by the company's promises of dramatic results with minimal surgery, all under local anesthesia. Any experienced plastic surgeon who performs facelifts could have told you that there was a vast disconnect between the Lifestyle Lift promises and the reallity of facial aesthetic surgery.
If you want to find out what happened to the Lifestyle Lift, click on the link below. It is a cautionary tale for patients seeking cosmetic surgery in the new millenium.
Check out Dr. Bosshardt's recent blog on hyperorlando House Calls.
Click on this link: http://www.hypeorlando.com/house-calls/2016/09/11/musings-on-an-early-morning-workout/#more-1509
For those women who feel they have suffered physical harm from breast implants and posted toxic reviews on my website and attacked me personally, please believe that I understand your anger and frustration. I cannot imagine what it is like to be hurting and feel that your situation is not being taken seriously. I feel, however, that I have been targeted unfairly and I hope you will read on and allow me to defend myself and my practice.
I have practiced medicine for nearly 36 years, both as a general surgeon and as a plastic surgeon. I have always tried to put my patient’s interests first and foremost. Have I always succeeded? No. I am not perfect and am not aware of any doctor who is. To say that I put profits before patients strikes at the heart of who I am and how I practice. I will not allow that accusation to go unanswered.
Check out Dr. Bosshardt's recent blog on hypeorlando House Calls.
Click on this link: http://www.hypeorlando.com/house-calls/2016/03/11/breast-implant-illness-the-bogus-controversy-that-just-wont-die/
Check out Dr. Bosshardt's recent blog on hypeorlando House Calls.
Click on this link: http://www.hypeorlando.com/house-calls/2015/08/18/in-case-you-wonder-why-your-doctor-is-frustrated-angry-discouraged-or-just-tired/

Learning is, by its very nature, a dynamic process. When you stop learning, it has the same effect on the brain that inactivity has on the body: decline. This is never more true than in the specialty of plastic surgery. The hard part is separating the hype from reality. Much that is promoted as “new” and/or “better” is largely marketing hype and an attempt to reap a financial windfall by being the first with the newest rather than true progress.
That said, the new buzz word in facial rejuvenation is “volume”. This has even spawned a new verb: volumizing. As we age, several things happen related to changes in our skin, fat, and muscles, and to the relentless effects of gravity. In the face we see wrinkling, sagging, and volume loss. The first two have been recognized for decades and have been addressed with a plethora of procedures ranging from chemical and laser skin peels to major surgery, e.g. facelifts. Volume loss has only been really addressed relatively recently.

In surgery, you canÂ’t always have your cake and eat it too. Doing any operation results in changes, e.g. a scar, that cannot be reversed and may affect the ability to do future surgery successfully. A striking example of this is cosmetic abdominal surgery using laser assisted liposuction.
Check out Dr. Bosshardt's recent blog on hypeorlando House Calls.
Click on this link: http://www.hypeorlando.com/house-calls/2015/01/13/its-a-new-year-now-what/
Check out Dr. Bosshardt's recent blog on hypeorlando House Calls.
Click on this link: http://www.hypeorlando.com/house-calls/2014/12/09/cosmetic-surgery-a-bogus-specialty/#.VIcttZveVmc.facebook
Check out Dr. Bosshardt's recent blog on hypeorlando House Calls.
Click on this link: 4 questions you should ask your plastic surgeon before he cuts on you and 2 that don't really matter
Different medical specialties often share some areas in common. One example would be hand surgery. General surgeons, orthopedic surgeons, and plastic surgeons all receive some training in hand surgery during their respective residencies. Some go on to specialize in this area. Skin cancer is another area that straddles specialties with general surgeons, plastic surgeons, and dermatologists all offering their services to patients with skin cancer. So, who should you go to?
Skin cancer, of course, is primarily a disorder of the skin and so it would seem obvious to go to a dermatologist for this. Dermatologists treat a lot of skin cancers and, indeed, some subspecialize in this area. Dermatologists can treat most skin cancers. They may offer freezing, burning, scraping, laser, and surgery. For the last one, dermatologists often use a technique called Moh’s surgery to remove skin cancers. This technique dates back to the 1930’s and is still considered the “gold standard” by the specialty.
The buzz word in facial rejuvenation today is "volumization". That may not actually be a real word but it does reflect an increasingly popular concern in facial rejuvenation. Traditional approaches to rejuvenating a face have taken one, or both, of two approaches: surgical tightening, such as with a facelift, or smoothing, done with chemical and laser peels. Both have their place and can provide substantial benefits to carefully selected patients.
One of the less appreciated changes that accompanies aging is volume loss. In our largely overfed and overweight culture, this is often overlooked because weight gain can mitigate some of the loss of fat in the face over the years. Many people, however, show obvious loss of fullness in their faces with aging. In those who maintain their weight at an ideal, this can even produce a "gaunt" or "severe" look to the face. The solution is to restore volume.
Twenty plus years ago, the only available commercial filler was collagen, derived from the hide of cows. 2% of the population was naturally allergic to this and so patients needed to have a skin test done before they could have collagen injections. While effective for filling small areas, cow collagen rarely lasted more than a couple of months, making it prohibitively expensive and impractical. With the advent of better fillers, cow collagen disappeared from the medical marketplace. Other forms of collagen, such as from human tissue banks, are still available but have not been popular.
Imagine this scenario. You go to a car lot to buy a car. The car salesman walks up (realizing that car salesmen don't have the best reputation, being just a few notches up from lawyers, politicians, and telemarketers, we'll assume this one is an upstanding sort).
"Hi, how may I help you?"
If you have had breast implants for 20 years or more, congratulations. You weathered the turbulent 90Â’s with the unprecedented media hysteria surrounding the concern of possible harm to womenÂ’s health from breast implants. Millions of women were needlessly frightened, some terrified, and many underwent unnecessary surgery to remove their implants after being told these would make them sick. It took over 10 years of good science and clinical studies to put these issues largely to rest. It was not one of the finer chapters in the history of my specialty. Unfortunately, the specter of cancer and disease muddied the waters and obscured the fact that there are real problems with breast implants.
I tell every patient who comes in to discuss possibly having implants inserted the same thing: inserting breast implants is an inherently unnatural thing to do and there are very real problems and downsides to having implants. I take great pains to inform women of these. It seems to only very rarely dissuade any of them from going forward. Such is the popularity of, and desire for, what implants can do. So, what are the problems with old implants?
Breast implants made two decades, or more, ago were made using technology available then. This may seem an obvious thing to say but it is important not to judge them based on what we know now. Back then, the goal was to make the implants feel as much like breast tissue as possible. Gel implants contained a very liquid, runny gel. When these implants developed even the tiniest hole, the gel would ooze out of them into the pocket around the implants. Some implants were made with a very thin shell and the silicone gel could even diffuse out through pores in the intact implant shell. This was called gel “bleed” and explained how some intact implants had sticky gel on the outside years later.
Size matters. I once had a body builder come in with an infected biceps implant. I don’t insert these as the complication rate is high and, personally, I just don’t like this type of surgery. I asked the fellow, whose biceps were already huge, why he had implants put in at all. His answer was telling. He said, “you know how it is, Doc, when you have 28 inch biceps, you want 29 inch biceps”.
Imagine for a second if Goldilocks, when she was older, had sought breast implants. After the first operation, she would have exclaimed, “these implants are too big!”. After a revision, she would have observed, “These implants are too small!”. After her exasperated plastic surgeon revised her yet a second time, hopefully she declared, “these implants are just right!”.
The holy grail of breast implant surgery is the augmented breast that looks and feels natural and is the perfect size for the individual. Focusing on the latter issue, what is the perfect size breast? The answer to this question is as varied as are the women who seek breast augmentation. What is perfect to one is too large for another and too small for yet a third individual. Figuring out what size implant to choose for a patient is a large part of the “art” of this procedure.
Keep It Simple, Stupid. This is something I tell myself all the time. The acronym K.I.S.S. is a reminder to never do something unnecessarily complicated when a simple solution will work equally well, or even better.
The training of a plastic surgeon includes in depth instruction in a wide variety of different grafts and flaps for reconstruction of defects produced by trauma, cancer treatment, and other 'misadventures' of life. Some of these are elegant and complex, and can salvage some very difficult reconstructive challenges. I once saw a patient who had undergone removal of a skin cancer on his cheek by a non-plastic surgeon. The scar gave clear testimony that the skin defect was reconstructed using a Lindberg Flap, named after the Russian surgeon who pioneered it.
A Lindberg flap uses skin and fat adjacent to the defect and has a trapezoidal shape. I have used them and, for certain defects, they work great. When former president Ronald Reagan had a skin cancer removed from his nose a Lindberg Flap was used to close the defect.
Many questions have a simple answer and a more complicated one. The simple answer to this question is: you canÂ’t, at least not precisely. The more complicated answer has to do with all the variables that come into play when discussing breast implants and size.
Most women know that when they buy bras of the same cup size from different manufacturers, they may not fit the same way. Different cup sizes from different manufacturers may fit the same. The reason for this, and what makes discussions of breast size so difficult, is that there is no standard for what an A, B, C, D, or other cup size really is. In a vault somewhere, in the National Bureau of Standards, there is a 12 inch ruler that is the standard for what 12 inches means. All rulers are made to that exact standard so that all 12 inch rulers are of identical length. No comparable standard exists for bra cup size. All manufacturers make bras to their own particular standards, which is why a B cup bra from one manufacture may fit you the same as a C cup from another.VictoriaÂ’s Secret bras are consistently smaller than other bras. I think this is to make their customers feel good that they can wear a C or D cup, when bras purchased elsewhere are B or C cups, respectively.
There are also multiple methods for measuring women for bra size and these can yield different cup sizes for the same person, further adding to the confusion.
If it involves a laser it must be better than a procedure without the laser, right? This is a common misconception which arises from our natural fascination with new technology. There is also an inherent desire in people ( or is it only Americans ) to be the first to experience the newest wrinkle, no pun intended, in plastic surgery. To understand laser resurfacing, one must know a little bit about lasers.
Laser. The word is an acronym and stands for Light Amplification by Stimulated Emission of Radiation . Laser light has several unique properties. It is monochromatic, that is, it contains only one color or wavelength of light. It is coherent, meaning that the light beam does not disperse with increasing distance from the source; the beam is focused, even at great distances. It is very powerful. The heat generated by some lasers is likened to that on the surface of the sun.
Lasers work by transmitting their energy to the material that they strike. If the material absorbs the laser light well, the laser light energy will transfer to the material which will heat up. The carbon dioxide (CO2) laser produces an invisible light which has a wavelength that is absorbed by water. When this light strikes a living cell, the laser energy is transferred to the water in the cell. If sufficient energy is transferred, the water in the cell will boil or vaporize, destroying the cell. In the past, CO2 lasers had limited usefulness in that a lot of their heat was transferred to areas around the target spot, producing too much collateral damage to tissues. The solution to this was pulsing. Pulsed lasers transmit an incredibly brief, incredibly powerful burst of laser light. On striking the skin, the first layer of cells is vaporized but before anymore underlying tissue can be damaged, the light has shut off. This allows the CO2 laser to resurface the skin, layer by layer, without producing a more extensive zone of injury, or burn. Although no longer a new technology, the pulsed CO2 laser is still the workhorse for skin resurfacing of the face and the results are the “gold standard” for this procedure. It does have the longest “down” time, leaves the skin quite pink for months, and is the most “invasive of the laser techniques.
Breast Augmentation- Information for Patients
The decision to have a breast augmentation is a major one with life-long consequences. Please be sure you understand this operation well and have all of your questions answered before proceeding. Once surgery is done, it can never be totally undone.
The only way to add meaningful volume or fullness to your breasts is to use breast implants. You cannot do exercises, take pills, use creams, or use “vacuum pumps” to accomplish this goal!! There is a technique, called fat grafting, in which fat is liposuctioned from your body and injected into your breasts. This technique is still not recommended for widespread use because long term results are not known and I am not yet offering it. It is not an option for thin patients. The following information is being provided to you in order to ensure that you are fully informed about breast augmentation with implants. It is a comprehensive summary of this very popular plastic surgical procedure. Together with your consultation with me, the information contained herein should allow you to make an informed decision about whether or not this operation is for you.
Breast Augmentation- Information for Patients
The decision to have a breast augmentation is a major one with life-long consequences. Please be sure you understand this operation well and have all of your questions answered before proceeding. Once surgery is done, it can never be totally undone.
The only way to add meaningful volume or fullness to your breasts is to use breast implants. You cannot do exercises, take pills, use creams, or use “vacuum pumps” to accomplish this goal!! There is a technique, called fat grafting, in which fat is liposuctioned from your body and injected into your breasts. This technique is still not recommended for widespread use because long term results are not known and I am not yet offering it. It is not an option for thin patients. The following information is being provided to you in order to ensure that you are fully informed about breast augmentation with implants. It is a comprehensive summary of this very popular plastic surgical procedure. Together with your consultation with me, the information contained herein should allow you to make an informed decision about whether or not this operation is for you.
 He was one of the two most influential men in my life; my father is the other. He was also one of the most influential men you never heard of. He passed away on Father’s Day. In a professional career spanning over 50 years, plastic surgeon D. Ralph Millard, Jr., MD, wrote or co-wrote 9 books, published 149 papers in peer-reviewed medical journals, and wrote 53 chapters in medical textbooks. He developed the operation used throughout the world today for the repair of cleft lips. He personally repaired thousands of cleft lips and palates.
He was one of the two most influential men in my life; my father is the other. He was also one of the most influential men you never heard of. He passed away on Father’s Day. In a professional career spanning over 50 years, plastic surgeon D. Ralph Millard, Jr., MD, wrote or co-wrote 9 books, published 149 papers in peer-reviewed medical journals, and wrote 53 chapters in medical textbooks. He developed the operation used throughout the world today for the repair of cleft lips. He personally repaired thousands of cleft lips and palates.
A supremely innovative surgeon with a lifelong thirst for perfection of his craft, he also developed numerous procedures and surgical instruments. He was an acknowledged master of one of the most difficult procedures in the specialty- total nasal reconstruction and his results sometimes looked better than the patientÂ’s original nose.
As impressive as these accomplishments were, perhaps his greatest professional legacy were the hundreds of residents and fellows that he trained in the science and art of plastic surgery over 28 years as head of the division of plastic surgery at the University of Miami/Jackson Memorial Hosptial. His list of students reads like a Who’s who of plastic surgery. Some have returned to their home countries to use what they learned to serve patients and, in turn, pass on this legacy to their own residents. In the U.S. many of Dr. Millard’s protégés have become heads of training programs and trained several generations of plastic surgeons. Anyone who has ever required the services of a plastic and reconstructive surgeon has benefited in some way from the influence of Dr. Millard.
Reduction mammaplasty, the medical term for a breast reduction, is one of the most common plastic surgery procedures. In my experience, it also has one of the highest rates of patient satisfaction of any procedure in the specialty. I think this is for two reasons: women with very large breasts are usually pretty miserable and appreciate the relief obtained and results are, aesthetically, usually pretty nice.
There is no “cookbook” formula for who is a candidate. If you have large, full breasts and are having symptoms from these, then you are probably a candidate. Cup size is not always helpful. While most women with problems with have bra cup size in the D and larger range, I have seen women with significant problems who wore a C cup.
I take a very comprehensive history when evaluating patients for breast reduction surgery. In addition to their cup size I want to know about any aches and pains in the back, neck, and shoulders. Problems with rashes under and between the breasts are common with large breasts. Some women complain of a “pulling” sensation on their chest and discomfort with laying down, as the large breasts spill to the sides. Numbness and tingling down the arms, into the hands and fingers, can be caused by large breasts. A physical examination, of course, will confirm that the breasts are large. I take detailed measurements and always document the size of the breasts with photographs. Very helpful is the presence of grooves in the shoulders where the bra straps dig in. This is an objective, tell tale sign of a problem.
What implant style should I choose?
It seems most patients coming into for a consultation for breast augmentation these days are doing a lot of research online before seeing a plastic surgeon. Among the various decisions that have to be made about implants is what style of implant to choose. Choices in both saline and gel implants include round/smooth, round/textured, tear drop/smooth, and tear drop/textured. Round implants are broken down even further into moderate, moderate “plus”, and high profile implants. How is a person to choose among these?
Let me explain texturing first. A ‘textured’ implant has a surface that looks and feels rough or fuzzy. This surface texturing is intended to encourage the attachment of the tissues around the implant to the surface of the implant. Think of a Velcro-like adherence. The idea behind this is that the surface texturing and tissue adherence will reduce the likelihood that the pocket around the implant might contract, squeezing the implant and making the breast feel hard and/or distorting the shape. This condition is called capsular contracture and is one of the main reasons some women get a less than perfect result. There are several issues with textured implants.
I am not above posting the comments of other plastic surgeons if I feel that they have something to say, and are saying it well. This post by Dr. Paul Howard, in Birmingham, Alabama, on liposuction is excellent, and very well written. I agree with everything in it. Dr. Howard is a board certified plastic surgeon and also an alumnus of the training program that I graduated from, in Miami, Florida, under Dr. D. Ralph Millard, Jr. Maybe great minds DO think alike! Just kiddingÂ…but, seriously, the post is well worth reading for anyone contemplating liposuction these days. It is so hard to separate the hype from the reality.
Check it out: http://liposuctionbirminghamal.com/
When the movie “Jaws 2? came out, the tagline was “just when you thought it was safe to go back in the waterÂ….. After the breast implant scare that surfaced in 1990 with the “expose” by Connie Chung, it was over 10 years before enough data was gathered around the world to confirm, to a medical certainty, that breasts implants did not make women ill, and did not put them at risk for breast, or any other cancer. Women returned to plastic surgeons offices in droves to have the implants put in that they had desired, but postponed, during media hysteria.  Unfortunately, in a distressing nod to Jaws 2, it can be said: “just when you thought it was safe to get back into the plastic surgeonÂ’s officeÂ….. Now, there is new data suggesting a possible association between implants and a very rare cancer.Â
Medical certaintly is not the same as 100% sure. For one thing, it is not possible to prove a negative. No one can prove now and forever that breast implants do not cause cancer because there is always the hypothetical possibility that some woman, some where, under just the right set of circumstances, may experience just that. All it takes is one case to blow medical certainty out of the water.
Medical knowledge is not static. It is constantly changing as new information is discovered. Doctors can only practice according to what knowledge is available at the time. Until recently, there has been no connection observed between women having breast implants and increased risk of any cancer.
It seems the Lifestyle Lift has become very popular and we get a lot of questions about this procedure. I canÂ’t tell you much about this procedure specifically. The reason is that this is a proprietary surgical procedure. This means that the doctor who developed it, David Kent, D. O., an otolaryngologist, has registered the Lifestyle Lift as a trademark and the only way a physician can learn details about it is to pay him for the privilege. It costs several thousand dollars to take his course and learn how to perform the Lifestyle Lift. However, as a plastic surgeon with 21 years of experience I can tell you some things based on having seen patients who have had this procedure done. As a plastic surgeon, I perform facelifts frequently. I am familiar with the different types of facelifts and variations of this procedure, I know the anatomy well, and the changes that occur with aging which a facelift is intended to correct. I also know the limitations of the procedure. Â
The Lifestyle Lift is a variation on a mini-facelift. Mini facelifts differ from full facelifts in that there is much less cutting and releasing of the skin from the underlying muscles. Less skin is removed. The surgery takes less time, carries fewer risks, and recovery is quicker. All good, right? The problem is that the results are less too. The surgeon who trained me, Dr. D. Ralph Millard, Jr., who performed many thousands of facelifts in his 40+ year career said it best: “Mini procedures give mini results”. I think this is as true today as when I trained over 20 years ago.
The Lifestyle Lift brochures and web site are very impressive and show results that border on the unbelievable. It has been my experience that when something sounds too good to be true, it usually is. Looking at the Lifestyle Lift a little more closely there are some things that just don’t sound right. On the one hand, the procedure promises incredible results with an hour of surgery. This is pushing things even for a mini-facelift. The brochures and web site, however, also state that many of the patients underwent an additonal “neck firming” procedure. What was that? The brochures and ads don’t say. I can tell you from some former Lifestyle Lift patients that their surgery took a lot longer than an hour and more than a week to recover from. None of the results that I have seen have been remotely as impressive as what I see on the brochures and several patients were very unhappy with their experience as the doctor did not spend much time with or explain the procedure well, and they did not get the results promised.
 Many patients ask me about bras after they have had breast augmentation surgery. As I tell every patient who comes in seeking this enhancement, breast augmentation is an inherently unnatural thing to do. Breast implants, while good, are not perfect in duplicating what is naturally missing so the final result will rarely look and/or feel 100% “natural”, although very nice none-the-less. One aspect of this “unnaturalness” (is that a word?) will be how the augmented breasts fit into a bra. Fitting for bras normally can be a challenge. Trust me on this: there is no standard out there for cup size. If you buy the same cup size from ten different manufacturers, they will all fit you differently. I do not use bra cup size as a measure of breast size because there is so much variation. There are numerous formulas for fitting bras and they may give very different results. Victoria’s secret, for example, will size most women a full cup size large than anyone else. I think they feel this makes their customers feel better. When performing breast augmentation I try to use an implant size that will achieve a result that will satisfy my understanding of the patient’s desires, make them look as natural as possible, produce a visible increase in fullness, and, hopefully, avoid unnecessary problems for them, now and in the future. Women often don’t realize that the result will be with them for years, or even the rest of their lives, and I try to look down the road. But, I am getting off track. Back to bras……..
Many patients ask me about bras after they have had breast augmentation surgery. As I tell every patient who comes in seeking this enhancement, breast augmentation is an inherently unnatural thing to do. Breast implants, while good, are not perfect in duplicating what is naturally missing so the final result will rarely look and/or feel 100% “natural”, although very nice none-the-less. One aspect of this “unnaturalness” (is that a word?) will be how the augmented breasts fit into a bra. Fitting for bras normally can be a challenge. Trust me on this: there is no standard out there for cup size. If you buy the same cup size from ten different manufacturers, they will all fit you differently. I do not use bra cup size as a measure of breast size because there is so much variation. There are numerous formulas for fitting bras and they may give very different results. Victoria’s secret, for example, will size most women a full cup size large than anyone else. I think they feel this makes their customers feel better. When performing breast augmentation I try to use an implant size that will achieve a result that will satisfy my understanding of the patient’s desires, make them look as natural as possible, produce a visible increase in fullness, and, hopefully, avoid unnecessary problems for them, now and in the future. Women often don’t realize that the result will be with them for years, or even the rest of their lives, and I try to look down the road. But, I am getting off track. Back to bras……..
My advice regarding post operative bras is to wear comfortable sports bras, without underwires or thick seams, for the first month or so after surgery. The breasts may be sensitive and the implants will not have fully settled, so fitted bras will probably not fit well, underwires may be uncomfortable, and sizing may be inaccurate. Once the implants have settled and the breasts assumed their final shape, that is the right time to get fitted. The bottom line is that the best bra for you is the one that fits you well and gives good support. This may require a little trial and error. Most large department stores and lingerie stores have people trained to fit customers for bras. Admittedly, some women just happen to have that combination of chest circumference and breast shape/size that makes them very difficult to fit after breast implant surgery. There is one brand, Le Mystere (www.lemystere.com), that makes bras specifically for women with implants. The are a bit wider along the curve of the underwire and have some other modifications to better fit these individuals. They are available in many department stores, such as Macy’s and Neiman Marcus. They are not cheap at $76 each but if they are your best fit, they are worth it.
Sports bras are great but some don’t give enough support for women with larger breasts. One of my patients is a runner. A week after her augmentation, she ran 20 miles in a long distance relay! I don’t recommend this, but she was committed and did not have any problems. She searched extensively and came up with two sports bras that she felt were excellent. One is the Enell sports bra (www.enell.com) and the other is the “Tata Tamer” (no, I am not making this up) (www.lululemon.com). She states that both were extremely comfortable and gave “the girls” great support when she ran.
(This appeared as one my columns in the Orlando Sentinel in January 2001)
Q: A recent article in the paper was about a 15 year old girl who was seeking breast enlargement surgery with her motherÂ’s blessing. There seemed to be a lot of concern about this, presumably because of her young age. Is there a minimum age for plastic surgery?
A: The answer to this question depends on whether you are speaking of cosmetic or reconstructive surgery and must take into consideration both physiologic and psychological concerns. Reconstructive surgery is done routinely on children and even infants. Timing in such cases, however, is crucial. An excellent example is the repair of cleft palate. In this deformity, the two halves of the roof of the mouth fail to fuse leaving a gap which typically affects the muscles of the soft palate. Because there is no separation between the mouth and nose, food and liquid can go up into the nose when the infant eats. In addition to this, speech cannot develop normally since an intact palate is essential for normal speech.
Breast lifts and breast implant surgery are totally different procedures that do very different things. They can complement each other in that some patients need both but how does one know which is best for her? Ptosis, the medical term for sagging, is defined by the position of the nipple relative to the crease under the breast. You can do a very simple test to see if you have this. You may have heard of the “pencil test” for breast sagging. Lift up on your breast with one hand, place the pencil horizontally under the breast, right in the natural crease, and then let the breast go. Release the pencil and if it falls, there is no ptosis. If the breast holds the pencil in place, then there is some element of ptosis. If the pencil is held, note the position of the nipple. If the nipple is above the level of the pencil, then you have a “deflated” breast, called pseudoptosis. This is common in women who have breast fed and lost volume in their breasts. If the nipple is at the same level as the pencil, you have grade I ptosis. If the nipple is below the pencil, you have grade II, and if the nipple is the lowest point on the breast (sometimes referred to as a “National Geographic” breast, from all the photos in that magazine of women in primitive cultures who have never seen a bra and whose breasts point to the ground!), you have grade III. Breasts with pseudoptosis and grade I ptosis usually do not need a breast lift and will do well with just adding more volume, i.e. a breast augmentation with implants.
Women with grade II and III need a breast lift, called a mastopexy. Putting implants alone in such breasts usually produces a less than aesthetic result because now you will have a big, droopy breast. Some women can accept this to avoid the scars and expense of a lift, but it is not ideal. A mastopexy is a terrific procedure which will produce a “perky”, non-saggy breast. The down side of this is that it is a fairly extensive procedure, takes longer to perform than a breast augmentation), and leaves additional scars. At a minimum, there will be a scar along the margin of the areola. Additional possible incisions may leave a vertical scar from the areola to the crease under the breast and a scar along the crease itself. In most cases, the aesthetic improvement is worth the scars. The lifted breast will be more compact, because skin is removed, and therefore you may not fill out your bra as well as before and you might even go down a cup size.
Breasts that just need volume do beautifully with implants. See my earlier blog which is an online breast consultation to read details of this surgery. Sometimes, patients need both procedures because of sagging AND loss of volume, the double whammy. In those cases, I recommend doing the lift first followed by the augmentation 3 or more months later. I feel it is easier and safer to do the lift first. Some patients may find that after the lift, they are content and do not go on with the implant surgery. I usually try to dissuade patients from doing lifts and implant surgery simultaneously. These two operation work directly counter to each other. The lift is tightening the breast and making it more compact; the augmentation is trying to expand the breast out and make it bigger. Each operation raises the risks of complications from the other. Inevitably, some compromise will be required. Either the lift and/or the augmentation may have to be underdone to avoid the potential for postoperative complications. The cost savings and savings in time for recovery from doing these operations simultaenously is not worth the added risks and compromise in the procedures. It is usually safer and better to do them as a two stage process. There are exceptions, however.
Phone: (352) 742-0079
Fax: (352) 742-0059
Address:
1879 Nightingale Lane, Suite A-2
Tavares, FL
West of Waterman Hospital, just off US 441
No upcoming events found.
Sign up for newsletters from Bosshardt & Marzek, including news and information, current specials and upcoming events.
Dr. Richard Bosshardt has been recognized as a Florida Top Doctor for 2020.

Dr. Peter Marzek has been recognized as a Castle Connolly Top Doctor for 2020.

Dr. Richard Bosshardt recently celebrated 30 years as a member of the American Society for Plastic Surgeons.
![]()